


 Sign Out
Sign Out



If the stroke is caused by embolism, enoxaparin must not be administered for 72 hours following the event. The efficacy of curative doses of LMWH has however not yet been established, regardless of the cause, extent or clinical severity of cerebral infarction.
Acute infectious endocarditis (except for some emboligenic cardiac conditions).
Mild to moderate kidney failure (creatinine clearance between 30 and 60 ml/min).
In addition, in subjects of any age, curative doses of this medicinal product are generally not advisable when combined with the following (see Interactions): Acetylsalicylic acid at analgesic, antipyretic and anti-inflammatory doses; NSAIDs (systemic use); Dextran 40 (parenteral use).
This medicinal product is generally not advisable at prophylactic doses in the following cases: In patients with severe renal failure (creatinine clearance of approximately 30 ml/min as per the Cockcroft formula) (see Precautions for use: Renal function as follows); During the first 24 hours following intracerebral hemorrhage.
In addition, in subjects over 65 years of age, prophylactic doses of this medicinal product are generally not advisable when combined with the following (see Interactions): Acetylsalicylic acid at analgesic, antipyretic and anti-inflammatory doses; NSAIDs (systemic use); Dextran 40 (parenteral use).
Precautions for use: Do not administer by the intramuscular route; Hemorrhage.
The recommended dosage regimens must be respected (dosage and duration of treatment). Failure to comply with these recommendations can lead to hemorrhage, particularly in high-risk patients (the elderly, patients with renal failure, etc.).
As with other anticoagulants, bleeding may occur at any site (see Adverse Reactions).
If bleeding occurs, the origin of the hemorrhage should be investigated and appropriate treatment instituted.
Serious hemorrhagic events have been reported in the following situation: elderly subjects, particularly due to age-related renal impairment; patients with renal failure; bodyweight below 40 kg; treatment lasting longer than the recommended mean duration of ten days; non-compliance with treatment recommendations (particularly treatment duration and dose adjustment based on bodyweight in curative treatment); co-administration with drugs increasing the risk of hemorrhage (see Interactions).
Enoxaparin sodium, as with any other anticoagulant therapy, should be used with caution in conditions with increased potential for bleeding.
In any event, special monitoring is essential in the elderly and/or patients with renal failure, as well as during treatment prolonged beyond ten days.
Elderly patients (especially patients eighty years of age and older) may be at an increased risk for bleeding complications with the therapeutic dosage ranges. Careful clinical monitoring is advised.
Assay of anti-Xa activity may in certain cases be useful in detecting drug accumulation (see Laboratory tests as follows).
Mechanical prosthetic heart valves: The use of Enoxaparin Injection in the prevention of thromboembolic events in patients with mechanical prosthetic heart valves has not been specifically investigated. However, some isolated cases of thrombosis have been reported in patients with this device who received enoxaparin as prophylactic treatment of thromboembolic events. Confounding factors, including underlying disease and insufficient clinical data, limit the evaluation of these cases. Some of these cases were pregnant women in whom thrombosis led to maternal and fetal death. Pregnant women with prosthetic heart valves may be at higher risk for thrombo-embolism (see Use in Pregnancy: Pregnant women with Mechanical prosthetic heart valves under Warnings).
Renal function: In patients with renal impairment, there is an increase in exposure of enoxaparin sodium which increases the risk of bleeding. Since exposure of enoxaparin sodium is significantly increased in patients with severe renal impairment (creatinine clearance <30 ml/min), a dosage adjustment is recommended for therapeutic and prophylactic dosage ranges. Although no dose adjustment is recommended in patients with moderate (creatinine clearance 30-50 ml/min) and mild (creatinine clearance 50-80 ml/min) renal impairment, careful clinical monitoring is advised.
Before low-molecular-weight heparin treatment is initiated, it is essential to evaluate renal function, particularly in subjects 75 years or older, by determining creatinine clearance (Clcr), using the Cockcroft formula and based on a recent bodyweight measurement: In male patients: Clcr = (140-age) x weight/(0.814 x serum creatinine) where age is expressed in years, weight in kg and serum creatinine in μmol/l.
This formula must be adjusted for female patients by multiplying the result by 0.85.
When serum creatinine is expressed in mg/ml, the value should be multiplied by a factor of 8.8.
The following dosage adjustments are recommended for therapeutic dosage ranges: See Table 3.
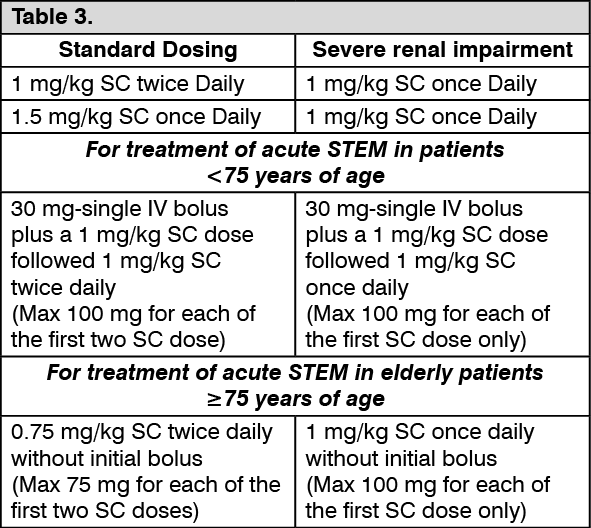 Click on icon to see table/diagram/image
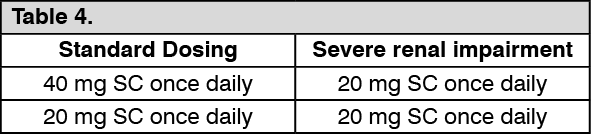
Click on icon to see table/diagram/imageThe following dosage adjustments are recommended foe prophylactic dosage ranges: See Table 4.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHepatic impairment: In the absence of clinical studies, caution should be used in hepatically impaired patients.
Low weight: An increase in exposure of enoxaparin sodium with prophylactic dosages (non-weight adjusted) has been observed in low-weight women (<45 kg) and low-weight men (<57 kg), which may lead to a higher risk of bleeding. Therefore, careful clinical monitoring is advised in these patients.
Obese Patients: Obese patients are at higher risk for thromboembolism. The safety and efficacy of prophylactic doses in obese patients (BMI >30 kg/m2) has not been fully determined and there is no consensus for dose adjustment. These patients should be observed carefully for signs and symptoms of thromboembolism.
Laboratory tests: Platelet monitoring: Heparin-induced thrombocytopenia (HIT): There is a risk of serious, occasionally thrombogenic, heparin-induced thrombocytopenia (reported with unfractionated heparin and less often with LMWH) of immunologic origin, called type II HIT (see Adverse Reactions).
As a result of this risk, platelet counts must be performed regardless of the therapeutic indication and the dose administered.
Platelet counts must be performed before administration or at the latest within 24 hours of initiating treatment, then twice a week during the usual treatment duration.
Should long-term treatment prove necessary in certain specific cases i.e. hip surgery, second and third trimesters of high-risk pregnancy (see Use in Pregnancy & Lactation), the schedule for platelet counts is twice a week during the first month of treatment (highest risk period) and then once a week until treatment discontinuation.
HIT should be suspected when the platelet count is below 100,000/mm3 and/or when there is a drop of 30% to 50% between two successive platelet counts. HIT mainly develops 5 to 21 days after heparin treatment is instituted (with a peak incidence after about 10 days).
This complication can however occur much earlier in patients with a history of heparin-induced thrombocytopenia, and isolated cases have been reported after 21 days. This type of patient history must therefore be systematically investigated by means of an in-depth interview before starting treatment. Furthermore, the risk of recurrence when reinstituting heparin may remain for several years or even indefinitely (see Contraindications).
In all cases, the occurrence of HIT constitutes an emergency situation and requires a specialist opinion.
Any significant drop in the platelet count (30% to 50% versus baseline) is a warning sign even before values reach a critical level. Should a decrease in platelets be observed, the following must be performed in all cases: an immediate platelet counts for verification; discontinuation of heparin treatment, if the drop is confirmed or even increased based on these results and when no other obvious cause is identified. A sample must be taken using a citrate tube in order to perform in vitro platelet aggregation and immunological tests. However, under these conditions the immediate measures to be taken are not based on in vitro platelet aggregation or immunological test results as only a few specialized laboratories perform these tests routinely and the results are available at best after several hours. These tests are however necessary to assist in diagnosis of the complication as the risk of thrombosis is very high if heparin treatment is continued; prevention or treatment of HIT-related thrombotic complications.
If continued anticoagulant therapy appears to be essential, heparin must be replaced by an antithrombotic agent of a different group such as sodium danaparoid or hirudin, prescribed at curative or preventive doses on a case-by-case basis.
Replacement by oral anticoagulants can only take place after the platelet count has reverted to normal due to the risk of exacerbation of thrombosis by oral anticoagulants.
Replacement of heparin by oral anticoagulants: Clinical monitoring and laboratory tests (prothrombin time expressed as the INR) must be intensified to monitor the effect of oral anticoagulants.
As there is an interval before the oral anticoagulant reaches its maximum effect, heparin therapy should be continued at a constant dose for as long as necessary in order to maintain INR within the desired therapeutic range, for the indication in two successive tests.
Monitoring of anti-factor Xa activity: As most of the clinical studies which demonstrated the efficacy of LMWH were conducted using a dose based on bodyweight without specific laboratory monitoring, the usefulness of laboratory tests for assessing the efficacy of LMWH treatment has not been established. However, laboratory tests, i.e. monitoring of anti-Xa activity may be useful in managing the risk of bleeding in certain clinical conditions often associated with a risk of overdose.
These situations mainly involve the curative indications of LMWH, due to the doses administered, in patients with: mild to moderate renal failure (creatinine clearance of approximately 30 ml/min to 60 ml/min calculated using the Cockcroft formula). As LMWH is primarily eliminated by the renal route, unlike standard unfractionated heparin, any renal failure can result in relative overdose. Severe renal failure is a contraindication to the use of LMWH at curative doses (see Contraindications); extreme high or low bodyweight (thinness or even cachexia, obesity); unexplained bleeding.
In contrast, laboratory monitoring is not recommended at prophylactic doses if the LMWH treatment complies with the therapeutic recommendations (particularly treatment duration), nor during hemodialysis.
To detect possible heparin accumulation following repeated administration, it is recommended, if necessary, to collect a blood sample at peak activity (based on available data), i.e. approximately 4 hours after the third injection when the drug is given as 2 subcutaneous injections per day.
Repeating anti-Xa activity assays to determine blood heparin levels, for example every 2 to 3 days, should be decided on a case-by-case basis, depending on the results of the preceding assay, and a possible LMWH dose adjustment should be considered.
The anti-Xa activity observed varies for each LMWH and each dosage regimen.
For information, based on available data, the mean value (± standard deviation) observed 4 hours after the 7th injection of enoxaparin given at a dose of 1 mg/kg/injection b.i.d. was 1.20±0.17 anti-Xa IU/ml.
This mean value was observed during clinical trials for anti-Xa activity assays carried out by a chromogenic method (amidolytic).
Activated partial thromboplastin time (aPTT): Some LMWHs moderately increase aPTT. As no clinical relevance has been established, monitoring of treatment using this test is of no use.
Situations involving particular risk: Monitoring of treatment should be intensified in the following cases: hepatic insufficiency; history of gastro-intestinal ulcers or any other organic lesion likely to bleed; Chorioretinal vascular disease; post-operatively, following cerebral or spinal cord surgery; lumbar puncture: this should only be considered taking into account the risk of intra-spinal bleeding and should be postponed whenever possible; concomitant use of medicinal products affecting hemostasis (see Interactions).
Effects on ability to drive and use machine: Enoxaparin sodium has no effect on the ability to drive and operate machines.